Profit Pump: 100 years after first patient uses insulin, out-of-pocket costs continue to climb
Manufacturers, insurance industry trade barbs while those with diabetes face impossible choices
InvestigateTV - Every day, usually multiple times a day, millions of people in the U.S. put into their bodies a substance that per milliliter is 60 times more expensive than a bottle of 2008 vintage Dom Perignon champagne.
Whether it’s drawn into a syringe, dialed up by a pen or dosed by an automatic pump, the chain of proteins known as insulin is required by those diabetes patients using it to stay alive.
For many patients, however, the cost of survival is at an all-time high — despite the life-sustaining drug marking 100 years of human use in January.
Pharmaceutical companies blame the cost on insurance companies and “middlemen” for not passing along savings, while those insurance companies and contractors say it’s the drug makers that ultimately set the price.
While lawmakers at both the state and federal level have attempted caps on copays or taken the companies to court over business practices, patients say many in the diabetes community are forced to choose between paying their bills or rationing their medication — and the results can be deadly.
‘It’s terrifying’
Megan Cornelius has carved out a sizable following on social media, but not about her job in tech start ups or life in Southern California.
Instead, her channel focuses on the diagnosis she received when she was 10 years old.
“I actually self-diagnosed myself,” she said, recounting how a childhood friend had received the news of having Type-1 diabetes and she recognized the symptoms in herself.
“I just remember sitting there crying and saying, ‘Can I eat pizza? Can I eat cake?’” she said.
As an adult with Type-1, she said she still must carefully consider what she eats each day, but it takes much more mental energy thinking about the financial implications of her disease.
“It’s terrifying, because in America, our insurance is tied to our jobs. If you lose your job at any moment, you could just be out-of-luck getting insulin,” she said. “If I got fired right now, next month, I might not have enough money to afford what I need to live.”
The financial strain and emotional toll led her to create a platform aimed at supporting other patients with diabetes by not only sharing tips on how to save money or navigate the health care system, but by reminding them they are not alone.

Cornelius said based on everything she’s learned about living with diabetes she considers herself lucky — because of her stature she only needs about a vial and a half of insulin each month, compared to others who may need five or more. With insurance her out-of-pocket cost for insulin is just $35 per month — and her insurance plan covers up to 90% of her other diabetes medications and supplies, such as her pump and blood-glucose monitor.
But that’s after she meets her $1,500 deductible, which she said she does in the first week or two of each January.
Without insurance, she said the list price for her insulin and the supplies for her glucose monitor and pump averages around $6,200 every three months. Add in other medications to help regulate her blood sugar, visits to the doctor and other supplies, and Cornelius estimates treating her Type 1 diabetes would cost nearly $50,000 if she were uninsured.
Even with her insurance, she estimates she pays up to $10,000 out of pocket each year to manage her disease.
She said she has experienced the fear of not knowing if she can afford it all.
“First time I was laid off from a job, literally, that was the first thought: ‘How am I going to afford to pay for my diabetes?’” she said.
Between the delay in unemployment benefits and the limitation of the affordable plans on the healthcare marketplace, she was stuck having to cobble together the cash for her medication.
“I found a ton of odd jobs to make it happen,” she said.
She added that thanks to her physician prescribing the maximum dose she would ever need per-day, she had some reserves of insulin as well.
“I had a little bit of a supply leftover so I could make it through until I was able to figure out what to do for insurance and how I could afford it,” she said.
Others in the same situation, however, are not always as fortunate.
The American Diabetes Association estimated in the summer of 2020, even as COVID-19 unemployment and wage-losses finally began to drift back down, more than 650,000 diabetes patients in the U.S. were still regularly rationing their insulin by skipping doses or taking less than prescribed. The ADA also estimated 3 million people were skipping blood glucose tests.
For diabetes patients reliant on prescribed insulin, but especially those with Type 1 diabetes, rationing the drug can be deadly.
When asked if she thinks people are dying because they cannot afford their insulin, Cornelius said there isn’t a doubt in her mind.
“1,000%,” she said. “I can think of a couple people on the top of my head that have died because of it.”
Prices Vary
What a patient pays at the counter for insulin varies greatly depending on if they are insured and what kind of policy they have, which pharmacy they are doing business with and which type of insulin they’ve been prescribed.
Three companies, Eli Lilly, Novo Nordisk and Sanofi produce 96% of the world’s insulin for human use.
InvestigateTV looked at the hallmark insulin from each of the three major manufacturers: Humalog from Eli Lilly, Novolog from Novo Nordisk and Lantus from Sanofi.
Those brands were also the three most prescribed to respondents to an informal survey conducted by InvestigateTV in 2021.
Doses of insulin are measured in “units,” with patients needing a daily amount based on their body weight as well as additional, smaller doses to account for carbohydrates in food or mitigate blood sugar spikes.
For example, a patient weighing 160 pounds could have a daily requirement of 40 units, plus additional doses at mealtimes.
Humalog and Novolog are both short-acting insulins, meaning they begin to lower blood sugar about 15 minutes after a dose, while Lantus is a long-acting insulin and works to lower blood sugar throughout the day. While all three are available in easy-to-use pens, the cheapest option is generally for a vial, with the most common being a 10 milliliter vial containing 1000 units.
Depending on if they are Type 1 or Type 2, their body size, hormone levels or other factors, a patient’s needs can vary, though most require more than one vial per month. Patients who are particularly insulin-resistant, such as those with severe Type 2 diabetes, can use six to seven vials a month or more.

Online tools such as NeedyMeds — a nonprofit founded in the 1990s to assist patients who struggle to afford their prescriptions — show the range of retail prices patients might find at the pharmacy counter for a 10 milliliter vial of each of the three major brands.
Those amounts are similar to what an independent pharmacy InvestigateTV spoke with found when looking up the price of vials from their wholesale distributor around the same time.
List prices of these insulins have been on a steady march upward.

A congressional report looking at medication costs found list prices for a vial of Humalog, Novolog and Lantus have increased 1,219%, 627% and 715% respectively since the drugs were launched. Humalog, which has seen the largest over-time increase, entered the market first in 1996. Novolog and Lantus launched roughly a decade later, but introduced their products at a price similar to that of Humalog at the time.
In a 2021 informal, online survey posted to social media by Gray Media Group television stations, InvestigateTV asked respondents to share if they had health insurance and what type, as well as the total they pay out of pocket each month for insulin.
Those with employer-provided insurance, representing the majority of those answering the survey, reported paying an average of $173 a month. That category also had the widest range of responses, with some saying they had no out-of-pocket cost, while others said they pay up to $1,600 a month.
Those on Medicaid or Medicare reported much lower out-of-pocket amounts, averaging less than $100.
But data from the Centers for Medicare and Medicaid Services shows the programs — and ultimately taxpayers — have been paying increasingly high amounts per claim.

A few survey respondents reported they utilize Walmart’s ReliOn insulin brands, which cost $25 to $75 a vial, and others said they used biosimilars or “authorized generics” produced by the three major companies.
In a statement in response to a request for comment from InvestigateTV, Eli Lilly said its 2019 introduction of an authorized generic or “non-branded” version of Humalog, Insulin Lispro, has effectively lowered the price “down to what it was in 2008.”
“In the past years, we have introduced multiple solutions that have progressively lowered the out-of-pocket cost for Lilly insulin,” the company said in the statement.
[See Eli Lilly’s full statement below]
Novo Nordisk, which did not return InvestigateTV’s invitation to comment, introduced its own authorized-generic, Insulin Aspart, shortly after Eli Lilly did in 2019, according to industry news reports. The Food and Drug Administration also approved a biosimilar for Lantus in 2019.
While these less-expensive options exist along with older, more-basic types of insulin, pharmacists and providers repeatedly told InvestigateTV that doesn’t mean they are necessarily a better option — effective doses of older types of insulin can be difficult to calculate, and “non-branded” insulins and biosimilars may not be covered by insurance or even available at a patient’s pharmacy.
In an interview with InvestigateTV about changes to a federal drug discount program, Anne Webster, an Illinois nurse practitioner of endocrinology, said when one of her patients was forced to use an older type of insulin because of cost, she had concerns about his body experiencing more extreme high and low blood sugar events.
“It wasn’t my first choice for him,” she said.
In their responses to inquiries from InvestigateTV, Eli Lilly and Sanofi both claim they have programs and mechanisms in place to provide their products at a lower cost to patients, regardless of their insurance.
“We have a suite of innovative and patient-centric savings programs that have launched in recent years to help people reduce their prescription medicine costs,” a Sanofi spokesperson said.
But the dollar amounts patients see either on their insurance benefits documents or are asked to pay at the register at the pharmacy are still outrageous to Megan Cornelius, the California content creator.
When she was diagnosed as a child 25 years ago, she said a vial of insulin cost her family less than $50. Today, she said she sees that vial ringing up at $350.
“People can’t afford that, especially if they’re uninsured or under insured,” she said.
Instead, some of them are traveling to Canada or Mexico, where the same vials of insulin are available for purchase at a fraction of the price.
Even as someone who can usually afford her medication, Cornelius said she’s done it herself.
“I’m 30 minutes from the border to Mexico. I went to a wedding and stopped by a pharmacy afterwards,” she said. “I paid $60 for a pen and a bottle of insulin. It took me five minutes, and I didn’t need a prescription. So tell me why: A 30-minute drive, I can buy two bottles of insulin for $60, and here that will cost me $700. It’s the exact same thing.”
‘Cost’ depends on who you ask
While the list price of medications like insulin can be determined with a little research, what an individual patient may see at the cash register is determined by contracts and negotiations that are shielded from public view.
The path prescription medications take through the healthcare system from those manufacturers to the end patient has grown more complicated as “middlemen” such as pharmacy benefit managers (PBMs) and wholesale distributors have entered the supply chain.

Manufacturers set a list price, known as a “Wholesale Acquisition Cost,” and sell insulin and other drugs to wholesale distributors, or in some cases pharmacies directly, either for the list price or at a slight discount. The distributors sell to pharmacies, and while there isn’t typically a large additional mark-up, distributors may use the original list price rather than the discounted price they received from the manufacturer.
In most cases, a patient purchases insulin at the pharmacy and pays an amount determined by their insurance — either a set copay or percentage of the list price determined by coinsurance, or the retail price charged by the pharmacy if the patient hasn’t met their deductible.
The pharmacy then sends a bill to the patient’s insurance and typically receives an additional dispensing fee.
If the patient’s insurance company contracts with a PBM, the insurer may get a rebate for the insulin, based on rebates the PBM received from the manufacturer and fees paid by the pharmacy.
The details of these rebates, fees and other aspects of relationships between PBMs, insurance companies, pharmacies and manufacturers are often opaque, but experts and lawmakers alike attribute much of the increase in what patients pay for insulin to these relationships.
So do the entities themselves — but each side points to the other as the problem.
Lisa Joldersma, senior vice president for policy and research for Pharmaceutical Research Manufacturers of America (PhRMA), said the industry blames high costs to patients on insurance companies not passing along the rebates they receive.
“Health insurers purchase insulin in quantity, they secure significant discounts,” said Joldersma, who focuses on public policy, state and insurance issues. “Unfortunately, too often they are choosing not to make those discounts available to patients at the pharmacy counter, and we think that’s just wrong.”
While she acknowledged list prices for insulin set by drug manufacturers continue to rise, she said the net price — what manufacturers ultimately receive at the end of the process — has plateaued and even decreased since the late 2000s.
“Our companies are delivering better insulin, more innovative, easier to use insulin than was available 15 years ago, actually at a lower cost than 15 years ago,” she said, but clarified: “When I say lower cost, I have to refer to the major purchaser of insulin in this country, which is health insurers.”
A study by the University of Southern California’s Leonard D. Schaeffer Center for Health Policy & Economics indeed found that in 2018, while the list price of 100 units of insulin topped $25, the net price manufacturers received was less than $10. That gap used to be smaller.

However, a drug pricing investigation by the Committee on Oversight and Reform released in December 2021 claims the pharmaceutical industry’s stance is relying too heavily on the decrease in net price.
“A drug’s net price does not account for uninsured patients, who cannot access the benefits of rebates negotiated by payers and may pay the full list price for drugs. In addition, because certain out-of-pocket costs borne by patients are based on a drug’s list price, when drug companies raise the list price, patients may face higher out-of-pocket costs even as supply chain rebates lower the aggregate net prices of some drugs,” the investigation report reads.
In other words: When list prices go up, patients pay more — especially if they are uninsured.
Joldersma countered by noting more people in the U.S. have health insurance than ever before thanks to the Affordable Care Act, and she reiterated PhRMA’s view that the responsibility for high out-of-pocket costs lies with insurers and their intermediaries.
“The manufacturers do set the price; that’s absolutely true,” she said. “But manufacturers also deeply discount their products, and they do that because they want the products to be more affordable for patients, and again, unfortunately, the significant discounts that manufacturers offer and provide on insulin products are too often being held by insurers, and by their intermediaries, and they’re not being passed along to patients at the pharmacy counter, and we think that’s wrong and needs to change.”
The motivation behind the discounted prices, however, is seen differently by those in Congress.
Higher prices, higher priority
A Senate Finance Committee report on insulin commissioned in 2019 by Sen. Chuck Grassley (R-Iowa) and Sen. Ron Wyden (D-Oregon) found evidence that those discounts or rebates were often motivated by companies either seeking preferred placement on formulary lists — a list of prescription drugs covered by an insurer, often determined by a PBM — or to avoid retaliation by insurers and PBMs in the form of exclusion from formulary lists.
Based on documents provided by manufacturers to the Senate committee, the report found one example where the board of Novo Nordisk decided not to decrease prices because of the financial downsides and expected pressure from insurers and their “middlemen.”
The report states: “The company believed that its decision to decrease list price could upset payers, and that many in the drug supply chain (e.g., wholesaler distributors, PBMs, and health insurers) would be negatively impacted financially and could retaliate against Novo Nordisk.”

As with the production of insulin, the PBM market has three major players of its own that are specifically noted by the Grassley-Wyden report: CVS Caremark, Express Scripts and OptumRx.
The report found these companies have “significant marketing power when negotiating rebates.”
The result of that marketing power, Joldersma said, are lower prices for insurers but “mark-ups” for patients because that savings isn’t being passed along.
“You have an entity a powerful entity that is effectively buying a product on sale, 70% off, 80% off, and then turning around and asking an individual, who is paying premiums for their health insurance, asking that individual to pay 100% of the undiscounted price of the medicine,” she said.
The insurance and PBM industries don’t see it that way.
Savings: All for one, or one for all?
InvestigateTV reached out to AHIP (America’s Health Insurance Plans), a trade and lobbying association for health insurers, to ask about the claims raised by Joldersma and lawmakers.
In response, a spokesperson sent a link to a statement on recent legislation in the House of Representatives regarding caps on the price of insulin, as well as an information sheet on the industry’s position on “point of sale rebates,” or the passing-on of savings referenced by PhRMA.
“Health insurance providers are Americans’ bargaining power, negotiating for lower drug prices for everyone. That includes negotiating rebates for drugs and maximizing the impact for all plan enrollees by passing on those savings directly to patients and consumers through lower out-of-pocket costs and premiums,” the information sheet reads. “Big Pharma argues that those savings should not be passed on to everyone through lower premiums and lower cost sharing. Instead, they believe rebates should only go to patients at the pharmacy counter. While this may sound attractive — or even fair — on its face, what drug manufacturers don’t mention is that rebates are only available for some drugs.”
In the statement in opposition to a bill passed by the House of Representatives that would cap insulin copays at $35 for those with commercial insurance, AHIP placed the responsibility for the price of insulin squarely on the shoulders of manufacturers.
“Insulin prices are too high because Big Pharma alone sets and controls the price.”
But Beth Caveness, the pharmacist who shared the prices from her distributors for insulin, told InvestigateTV she and others in her field consider the proliferation of insurance companies utilizing PBMs to be the primary driver of the ever-increasing price of not only insulins, but all drugs.
“No matter what you fill, no matter what you do, they’re going to come up with a new way to take money from you,” she said, referring to not just patients, but business owners like herself.
Operating an independent pharmacy, she said she often takes a loss on insulin prescriptions in particular, because even after adding a standard retail mark-up, PBM fees erase any profit.
“We sell it to a patient and think we’re going to make $20, and then three months later, four months later, you find out that that pharmacy benefit manager takes about $40,” she said.
Dr. Steve Miller, the recently-retired but longtime chief medical officer for Express Scripts, argued PBMs like the one he helped lead are trying to reduce prices — that by negotiating with pharmaceutical companies on behalf of health plans, more patients get access to lower prices than they otherwise would.
“What we do is we negotiate against those manufacturers to try to lower that price for people that are lucky enough to have good insurance,” he said.
At Express Scripts, some plans are also eligible for what the company calls a “diabetes care value program” that Miller said further leveraged the company’s relationship with insulin manufacturers.
“We said, why don’t we take the money that you’re putting into patient assistance programs, or copay cards or giveaway stuff? And let’s buy-down the copay to $25 for everyone regardless of how much insulin they use, regardless of what branded insulin they use,” he said.
The result is a more predictable amount for those with specific insurance plans, but Miller admitted it leaves out those who don’t have any insurance or whose plan doesn’t meet the program requirements.
While the other individual PBMs, CVS Caremark and OptumRx did not respond to a request for comment, a spokesperson for the Pharmaceutical Care Management Association (PCMA) , a trade and lobbying organization for PBMs, contacted InvestigateTV after receiving word from member companies about those requests.
The spokesperson sent links to online materials, as well as a written statement:
“We believe the key to reducing drug costs is increasing competition, including for insulin products. Unfortunately, tactics used by drug manufacturers to avoid competition, including ongoing patent extensions on insulin products, are a significant barrier to getting costs down even further for people with diabetes.
PBMs have introduced programs to cap, or outright eliminate, out-of-pocket costs for insulin and have stepped up efforts to help patients living with diabetes by providing clinical support and education, which help patients maintain their insulin regimens and lead healthier lives.”
Miller also pointed back to manufacturers as holding the controls for the market.
“Only one stakeholder sets the price of drugs, that’s the pharmaceutical manufacturers. They could choose to quit raising those prices, and so and so the idea that the prices keep going up, and it’s being forced upon them is not true. If they want to sell the drug for a lower price, we would be thrilled to do that.”
Lawmakers don’t entirely disagree.
The Oversight Committee investigation notes similar points to both AHIP and PCMA, stating “the three insulin companies have engaged in strategies to maintain monopoly pricing and defend against competition.”

Both that report and the Grassley-Wyden report also reference the practice of “shadow pricing” with regard to insulin.
The lawmakers list examples of shadow pricing — where companies raise the price of a similar good seemingly in lockstep, virtually eliminating any price reduction based on market competition and often without the increases being related to inflation or the cost of producing the goods — by all three major insulin manufacturers.
In both reports, lawmakers also claim pharmaceutical companies are not spending enough money on research and development to justify higher prices. The industry refutes this by pointing to the new types and methods of administering insulin that have emerged over the last 15 years — including long-acting insulins, insulin pens and inhaled insulins — as evidence the drug has advanced like any other, — and again Joldersma, from PhRMA, blamed insurers and PBMs.
“Our manufacturers who are delivering insulin, better insulin than we’ve ever had before are providing substantial discounts that insulin to the insurance companies who are paying the bill,” Joldersma said, “and we think it is awful, that insurance companies are choosing to use those dollars to use those savings for things other than reducing the cost of being insulin for a patient’s diabetes is too important.”
‘We’ve got to hold them accountable’
While manufacturers, insurers and PBMs embody the 1968 episode of the animated Spider-Man series “To Catch a Spider/Double Identity” that became a viral sensation in 2011, patients with diabetes who are dependent on insulin are facing difficult choices.
“What happens to these individuals, they end up using expired insulin, they don’t take the correct amount of insulin, or they don’t take it at all, and then the physical consequences are, again are devastating in that regard,” said Mississippi Attorney General Lynn Fitch.
Fitch filed a lawsuit in June 2021 against the three major insulin manufacturers as well as the three largest PBMs — a lawsuit that coming from a state attorney general was the first of its kind.
“There’s a scheme going on here, there’s a pricing scheme going on,” she said, “and we’ve got to make it affordable. And in order to do that, we’ve got to hold them accountable.”
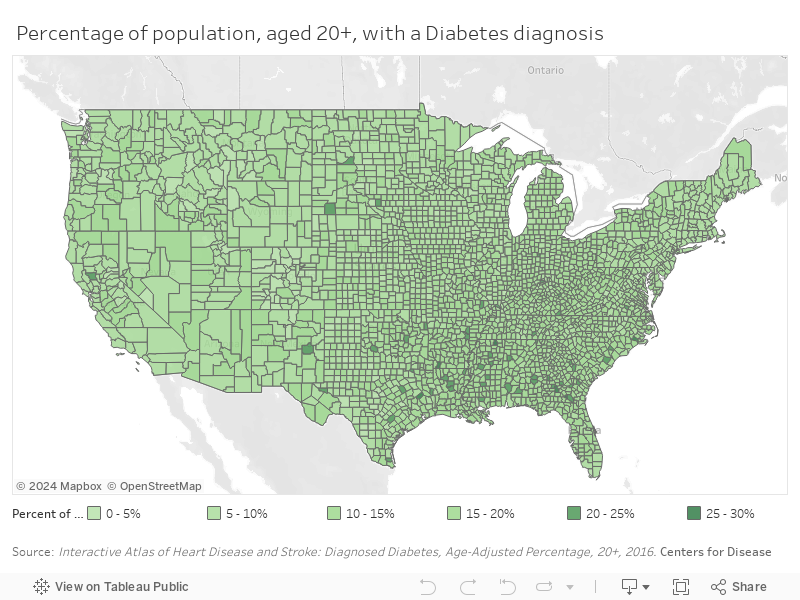
Mississippi, squarely in the “Diabetes Belt” has one of the highest rates of diabetes in the nation. In the Mississippi Delta, where socioeconomic factors also limit access to healthcare, around 70% of counties have a higher rate than the national average.
Fitch’s interest in the issue holds personal value as well.
“I’ve seen it, I have lived with my child going through these trials and tribulations and challenges,” she said.
Fitch’s daughter was diagnosed with Type 1 diabetes when she was 13.
“It just breaks your heart as a mother, ‘What could I have done differently? How did I not see this coming?’” she said of the questions that flooded her mind at the time. “But, you know, diabetes just sneaks up and says, I’m going to go in, and I’m going to affect this child’s life. And it truly did.”
She said the financial toll was significant as well, and remains on her mind even as her daughter has become an adult.
“It’s been a tremendous financial drain. From the moment she was diagnosed to the age she is now,” she said. “It’s devastating from the financial side.”
InvestigateTV obtained documents from the offices of 11 state attorneys general where patients filed consumer complaints involving insulin against both pharmaceutical companies and insurers.
A patient in Maryland alleged price gouging in early 2020 after their 90-day supply of insulin increased from $340 in February to $1,100 in March as the COVID-19 pandemic gripped the nation.
“This is the same year, same insurance plan, same prescription, and same pharmacy. When I spoke with my CVS Caremark representative, he said the manufacturers had increased the price significantly within the last month,” the patient wrote.
Fitch’s lawsuit, still moving through federal court, accuses the insulin manufacturers and PBMs of violating the Mississippi Consumer Act, unjust enrichment and civil conspiracy.
“The reason behind the increase [in insulin prices] is a fraudulent conspiracy between billion-dollar companies known as PBMs and the Manufacturer Defendants,” the complaint reads.
The complaint references an April 2019 congressional hearing where the state claims the defendants themselves explain how their interactions have driven up prices.
Fitch’s lawsuit faces an uphill battle, however.
Others against manufacturers, such as the one brought by the Minnesota Attorney General, have been either thrown out or gutted in federal courts, because in many cases federal laws don’t allow companies to be sued by an undefined plaintiff — and many cases are written as being on behalf of the entire population, not a specific person.
Those named in the lawsuit have filed motions to dismiss, claiming lack of jurisdiction and failure to state a claim.
Miller, with Express Scripts, couldn’t address specific litigation, but said he feels PBMs are being unfairly maligned.
“We have a system that’s created these high prices. And we have both regulatory legislative, but also market forces that are driving it up, we believe we’re the force for good trying to drive that down,” he said, adding, “all those things conspire to work against the patient, and we feel like we’re one of those forces to actually trying to do the opposite, but are often being blamed for the cause of high prices.”
Capping conundrum
Other efforts to curb the sticker shock patients face at the pharmacy counter, such as copay caps, have been slow going.
Several states have implemented or are in the process of debating caps on out-of-pocket spending on insulin for those with certain insurance coverage.
At the federal level, the House of Representatives passed its $35 copay cap on insulin prescription copays for the commercially insured — originally part of President Joe Biden’s “Build Back Better” plan — while on the other side of the hill Sen. Raphael Warnock (D-Georgia) and Sen. Susan Collins (R-Maine) have introduced and proposed, respectively, insulin price cap legislation.
Collins said in an interview with InvestigateTV that while caps are the primary topic of conversation on Capitol Hill, she does think more will need to happen to address insulin prices.
“I would agree that this is a far more complicated issue than just putting a monthly out-of-pocket cap on the amount that it’s paid for insulin, although that’s certainly it’s beneficial to many people,” she said.
“What I have found due to an investigation that was done when I was chair of the aging committee, is that the price of insulin is rife with conflicts of interest.”
The senator said those findings were similar to those from the Grassley-Wyden and Oversight reports: that manufacturers are keeping list prices high to be chosen by PBMs for an insurer’s formulary thanks to larger rebates, and PBMs not discouraging that behavior because their fees are based on a percentage of the list price.
Collins has not yet introduced her own bill, but according to Kaiser Health News has been selected along with Sen. Jeanne Shaheen (D-New Hampshire) to work on the Senate’s consideration of the House bill. Collins and Shaheen have previously worked together on insulin affordability legislation, but those efforts never saw a bill become law.
Manufacturers have in general been supportive of these attempts at capping copays for insulin.
A spokesperson for Sanofi, which produces the long-acting insulin Lantus, told InvestigateTV in an email: “Sanofi supports efforts to cap monthly co-pays for covered insulin. We also support legislation that results in patients paying less when they pick up their insulin such as requiring rebates to be shared at the pharmacy counter, requiring plans to cover insulin without applying a deductible, and prohibiting plans from imposing a higher co-pay than its net cost after manufacturer rebates.”
[See Sanofi’s full statement below]
Back in Southern California, Meagan Cornelius is skeptical of the effort in Washington, telling her TikTok followers the House bill is just “smoke.”
“They’re making people think they’re doing something, but they’re not,” she said in the short video.
Cornelius, who places the responsibility for the price of insulin squarely on pharmaceutical companies, said lawmakers should be more focused on regulations to reel in that industry, not legislate caps that don’t help all patients.
“Holding pharmaceutical companies accountable, putting caps on how they can raise prices, on the amount of money, they can actually make off a medication,” she said, listing what she thinks needs to change.
“The money their CEOs make is an unfathomable amount,” she said. “Cut that in half, what are you doing with all this money? Why do you need it so badly that you’re allowing people to die, just so you can have extra money in the bank? I don’t get it. I don’t get how someone can sleep at night with that.”
Justine Arens and Payton Romans provided research assistance for this report.
InvestigateTV reached out to the three major insulin manufacturers as well as the three pharmacy benefit managers referenced in congressional reports and lawsuits to address the claims made by various parties. Of those that responded, these were their full statements:
Sanofi:
List Price vs. Net Price
“Despite rhetoric about skyrocketing insulin prices, the net price (meaning the amount that Sanofi actually receives from a sale of its medicine after payment of any rebates or discounts on such sale) of insulin has been falling for seven consecutive years, making our insulins significantly less expensive for insurance companies.
PBMs have demanded rebates for pharmaceutical products for nearly two decades, and they are an engrained feature of our healthcare system. Since 2012, the net price of our insulins declined by 54%. Over the same period, the net price for commercial and Medicare Part D plans of our most prescribed insulin, Lantus, has fallen 62%, while average out-of-pocket costs for patients with commercial insurance and Medicare has risen approximately 60%. For all the focus by health plans and others on the growth of list prices, today, the average net price of Lantus is below 2006 levels.”
Sanofi Diabetes Access Programs
“We disagree with your claim that access to our patient programs are limited as we have a suite of innovative and patient-centric savings programs that have launched in recent years to help people reduce their prescription medicine costs.
• 100% of commercially insured people are eligible for co-pay assistance programs, regardless of income or insurance plan design, which limits out-of-pocket expenses for a majority of people between $0 and $10. These programs are available for those prescribed Adlyxin, Apidra, Lantus, Soliqua 100/33, and Toujeo.
• 100% of uninsured people are eligible for the Insulins Valyou Savings Program — regardless of income level — enabling them to buy one or multiple Sanofi insulins (Lantus, Toujeo, Admelog, and Apidra) for a fixed price of $99 per month, for up to ten boxes of SoloStar pens and/or 10 mL vials or 5 boxes of Toujeo Max SoloStar pens. Soliqua 100/33′s cash offer also allows uninsured people to pay as little as $99 per box of pens, for up to two boxes of pens for a 30-day supply.
• We also provide free medications to qualified low- and middle-income patients through the patient assistance component of the Sanofi Patient Connection program. Some people facing an unexpected financial hardship may be eligible for a one-time, immediate month’s supply of their Sanofi medicine as they wait for their application to process.
• Sanofi also volunteered to join the Centers for Medicare and Medicaid Services’ (CMS) Senior Savings Model which allows patients enrolled in participating Part D plans to pay a $35 or less co-pay for each 30-day prescription of a Sanofi insulin throughout the year.
The only people ineligible for our programs are those insured by federal programs, including Medicare and Medicare Part D, due to federal rules. Sanofi supports changes to these rules that would allow all patients to benefit from assistance programs.”
Pricing Allegations and Lawsuits
“We strongly believe the allegations have no merit, and we will defend ourselves against these claims.”
State and Federal Patient Out-Of-Pocket Caps on Insulin
“Sanofi supports efforts to cap monthly co-pays for covered insulin. We also support legislation that results in patients paying less when they pick up their insulin such as requiring rebates to be shared at the pharmacy counter, requiring plans to cover insulin without applying a deductible, and prohibiting plans from imposing a higher co-pay than its net cost after manufacturer rebates.”
Executive Compensation
“Sanofi executives’ compensation is not a factor in the Company’s decisions regarding the pricing of its medicines.
Consistent with our pricing principles, Sanofi sets the prices of its medicines based on their value, which includes considerations of the benefit to patients, compared to a standard of care; the reduced need — and therefore costs — of other health care interventions; and any increase in quality of life and productivity. We also consider factors such as the affordability for patients and any unique factors specific to the medicine, like the need to support ongoing clinical trials, implement important regulatory commitments, or develop sophisticated patient support tools that improve care management and help decrease the total cost of care.
Any price increases take into account these factors and also are limited to the projected annual health care spending growth rate — NHE — as estimated by CMS.
Moreover, Sanofi determines its executive personnel’s variable compensation based on a complex and multi-faceted set quantitative and qualitative criteria that account for both individual and company-wide performance and may include criteria related to research and development, new product launches, the financial performance of relevant business lines, organization and staff relations, and corporate social responsibility.”
Eli Lilly
Lilly is deeply committed to making insulin affordable for all people living with diabetes, regardless of income or insurance status.
In the past years, we have introduced multiple solutions that have progressively lowered the out-of-pocket cost for Lilly insulin. Today, anyone is eligible to purchase their Lilly insulin prescription for $35 or less per month, regardless of the number of pens or vials they use, and whether they are uninsured or use commercial insurance, Medicaid, or are enrolled in a participating Medicare Part D plan.
We have not raised list prices on any of our insulins for the past five years. To the contrary, we lowered the list price on our most commonly used insulin (Humalog) by 70%, bringing the list price down to what it was in 2008, by introducing our own non-branded equivalent and making it available to any health plan that wants to put it on their formulary.
Our solutions are making a real impact for people with diabetes. Despite rising deductibles, the average monthly out-of-pocket cost for Lilly insulin has dropped by 44 percent, to $21.80, over the last five years. This translates to $7-10 per vial and $2-3 per pen.
Lilly has been acting voluntarily to make its insulins more affordable for patients within our current healthcare system, but we also advocate for comprehensive solutions and public policies, such as passing through rebates directly to people who use insulin and limiting out-of-pocket costs, to move the U.S. healthcare system from a series of patchwork solutions to systemic change that helps people access and afford their insulin, and other lifesaving drugs.
None of our insulins’ active ingredients are patent protected, and we are not using patents to keep new entrants out of the insulin market. A follow-on version of Humalog has been on the market for four years. Lilly supports the use of generics and biosimilars to enter the market when patents rightfully expire. We also support removing regulatory barriers to allow such entry.
Scientists have made extraordinary strides in insulin innovation over the last 100 years, improving the lives of millions of people with diabetes. Lilly has pioneered many of the great advancements in insulin treatments, and our diabetes pipeline includes a once-weekly basal insulin medication that could eliminate daily insulin injections for certain individuals living with diabetes, and a “smart insulin” platform (glucose-responsive insulins that can sense sugar levels in the blood and automatically activate as needed throughout the day).
Until gaps in the healthcare system are filled, Lilly will continue to provide affordability solutions to people who need them. Anyone paying more than $35 per month for Lilly insulin can call the Lilly Diabetes Solution Center at (833) 808-1234 or go to insulinaffordability.com to learn more about our insulin affordability solutions and get help.
Additional facts on our Insulin Affordability Programs (also found on insulinaffordability.com):
Lilly has many programs that provide affordable insulin. In the past years, Lilly has introduced multiple solutions that allow people to purchase a monthly prescription of Lilly insulin for $35 or less, including:
• In 2020, we announced the Lilly Insulin Value Program, a co-pay card allowing people with commercial insurance or uninsured to buy their monthly prescription of Lilly insulin for $35. There is no application or enrollment process; interested individuals need only confirm they are over 18, a U.S. resident, and not covered by a government insurance program, and in a matter of seconds they will receive a copay card that they can download to their mobile device or print and present when they pick up their insulin prescription.
• Lilly and other manufacturers are contributing $250 million over five years to make our insulins available in the Senior Savings Model, allowing seniors in a participating Part D insurance plan to purchase their monthly prescription of Lilly insulin for $35.
• Lilly pays a 100 percent rebate to state governments to make our insulins available to millions of people in the Medicaid and VA programs.
• In 2019, we introduced a non-branded insulin, Insulin Lispro, at half the list price of branded Humalog. Insulin Lispro, which is the same molecule as Humalog, is now 70 percent off the list price of its branded counterpart.
Copyright 2022 Gray Media Group, Inc. All rights reserved.







